












Dehisced surgical wound – ICU
The 40-year-old patient with a recent diagnosis of oesophageal cancer had a 14 days old dehisced surgical wound following laparotomy and insertion of a gastrostomy tube for feeding. She was now in intensive care unit (ICU) after an in-hospital cardiac arrest. Furthermore, she had a low body mass index (BMI).
The wound had dehisced in several areas along the incision and therefore needed to be fully opened. The wound turned out to be 2 cm deep with an opening of 16 x 6 cm.
Amicapsil was applied a total of 4 times, i.e. on Days 0, 1, 2 and 4.
 |
 |
| Day 0 | Day 1 |
 |
 |
| Day 2 | Day 4 |
 |
 |
| Day 6 | Day 20 |
 |
|
| Day 57 |
On day 0, the wound was very sloughy and highly exuding and there were concerns over the possible presence of a small area of exposed bowel underneath the slough. After opening the wound fully to facilitate autolytic debridement, Amicapsil was applied for the first time.
Over Days 1 and 2, the exudate gradually reduced and was on Day 2 managed without the need of an absorbent dressing but only Amicapsil and a gauze. The wound edges were on Day 1 still dull and lifeless but on Day 2 they had contracted and were pink and healthy looking. There were patches of granulation tissue. The wound received the 3rd Amicapsil application and was revisited 2 days later.
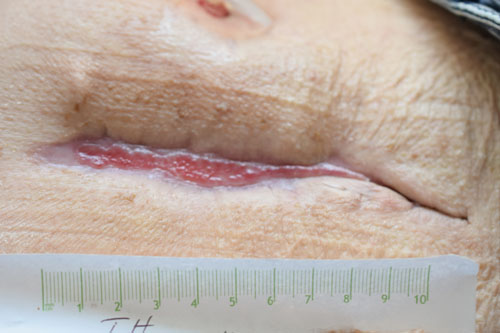
On Day 4, there were no signs of infection and very little moisture and slough. The wound had granulated and filled up from the bottom by 0.5 cm. This is easily visible by the increased coverage of the sutures. The wound edges now had good tension and were of a healthy whitish pink colour. The wound received the 4th and last Amicapsil application and was revisited 2 days later, i.e. on Day 6.
On Day 6, the slough was further reduced and the wound bed had granulated up from the bottom by further 0.8 cm so that the depth was now 0.7 cm. No Amicapsil was applied and the wound was revisited 2 days later.
From Day 8 onwards, the dressing was only changed weekly.
By Day 20, the patient had left ICU. The wound was fully built up with new soft tissue and all wound edges were actively epithelialising.
On Day 64 the wound was confirmed fully closed.
The responsible lead tissue viability nurse stated that she usually would have had to use Urgoclean for at least 7 days followed by NPWT for several weeks in order to get the wound to the clean state illustrated in the picture taken on Day 4.
She further pointed out that the pain during dressing changes was minimal.
Category IV pressure ulcer – coccyx area
A 58-year-old woman was hospitalised with a category IV pressure ulcer caused by lying on the floor for several days after a fall. Due to the location and depth of the wound, it was at high risk of infections, including osteomyelitis. The patient had an extensive history of alcohol dependence.
During the previous three weeks, several dressing types, including honey and superabsorbents, had been tried in an attempt to debride the necrosis and slough, with little success
The ulcer reached 3 cm down to the spine with an opening of 10 x 10 cm.
Amicapsil applied a total of 4 times: Days 0, 1, 2 & 3
 |
 |
| Day 0 | Day 1 |
 |
 |
| Day 2 | Day 3 |
 |
 |
| Day 14 | Day 64 |
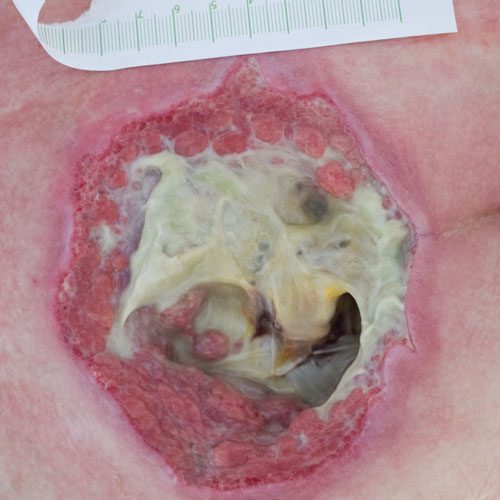
On Day 0, before the first Amicapsil application, the wound was very malodourous and heavily exuding.
On Day 1, there was a vast reduction in exudate, slough and odour.
On Day 3, the wound was completely debrided leaving the ligaments clean and visible at bottom. Granulation tissue was rapidly building up the tissue from the bottom of the wound and the edges were granulating very well; all leading to an overall 33% reduction of wound volume.
Amicapsil was applied one last time and, with this on, the patient was on that same day discharged to a community facility for rehabilitation.
The rehabilitation facility did not have access to Amicapsil. They chose to continue the care for the wound with TNP from Day 7, i.e. 3 days after discharge.
On Day 28, the patient was discharged from the rehabilitation facility to her home for the wound to be cared for by community care. They chose to continue the care for the wound with conventional dressings.
The wound healed; and at no point in the healing process was the wound readmitted with complications nor treated for any wound infections.
The responsible lead tissue viability nurse stated that wounds like these will regularly take several months to heal and cause the patients lots of complications generally associated with chronic infections and consequently with long hospital stays. Yet in this patient’s case the bottom of the wound was covered and the overall wound size reduced so quickly that this risk was reduced. She also pointed out that this particular wound was likely to have a long journey towards discharge and high risk of becoming chronic due to the patient’s extensive history of alcohol dependence.
Dehisced surgical wound – Lymph node dissection
The 57-year-old patient had undergone double-sided dissection of groin lymph nodes following a diagnosis of cancer.
The patient was originally discharged from hospital post-operatively but was later readmitted with lymphocysts to both groins and a dehiscence of the wound in the right groin.
Wound 1x1x1cm with a 3 cm deep sinus.
Amicapsil applied a total of 4 times: Days 0, 1, 2 & 3
 |
 |
| Day 0 | Day 1 |
 |
 |
| Day 2 | Day 5 |
On Day 0, the wound was very highly exuding and received its first Amicapsil application
On the following day, Day 1, the exudate had reduced considerably. Granulation was visible and the sinus had started to resolve. Also, the wound edges had cleared up.
On Day 3, there was no more discharge. The sinus had cleared and the granulation had filled up the cavity to a depth of less than 0.5 cm.
Amicapsil was applied a last time and patient was discharged home with this 4th Amicapsil cover on.
On Day 5, the wound was practically filled up with granulation tissue and the edges were epithelialising.
The wound healed up from the bottom with no signs of closing over at the top creating an abscess.
The patient was scheduled to start radiotherapy 2 weeks later and needed her wound to be fully healed in order for this to go ahead. This goal was successfully achieved.
The patient has had no further wound concerns after discharge.
The responsible lead tissue viability nurse stated that this was an example of a complication commonly seen in lymph node surgery. These wounds are typically very highly exuding and it would usually have been necessary to use NPWT for several weeks to manage exudate and until granulation would become visible.